Position Statement Recommendation
All people with cancer should be screened for malnutrition in all healthcare settings at diagnosis and repeated as the clinical situation changes, using a screening tool that is valid and reliable in the setting in which it is intended.
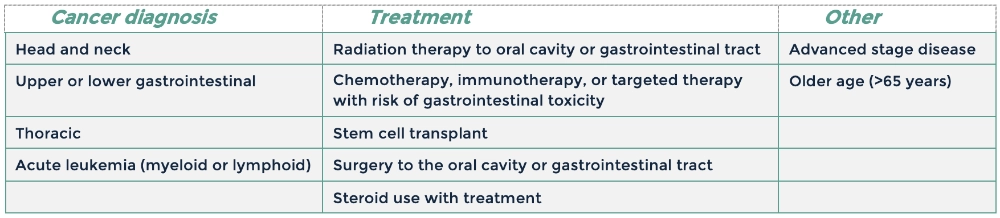
Screening for malnutrition can be bypassed for people with a cancer diagnosis or treatment plan known to lead to high risk of malnutrition (see Table 1).
Table 1. Factors indicative of high risk of malnutrition
The following malnutrition screening tools have been shown to be valid and reliable for identifying malnutrition in people with cancer. The table below summarises the settings in which each screening tool has been validated.
Table 2. Malnutrition screening tools
